Children with great vessel anomalies can exhibit a broad spectrum of symptoms. Some children may experience no symptoms, while others may have a range of symptoms that vary in severity. This depends on factors such as the specific type of anomaly and its impact on blood flow and surrounding structures. The timing of symptom onset also differs, with some children presenting symptoms at birth and others developing them later in life. Some common symptoms include:
- Respiratory issues: Difficulty breathing, rapid breathing, or wheezing, often due to compression of the airways.
- Feeding difficulties: Poor feeding, difficulty swallowing, or vomiting, which can be caused by compression of the esophagus.
- Heart murmur: An abnormal sound heard during a heartbeat, indicating turbulent blood flow.
- Cyanosis: A bluish tint to the skin, lips, and nails due to low oxygen levels in the blood.
- Poor growth or failure to thrive: The child may not gain weight and grow at the expected rate.
- Fatigue or lack of energy: The child may tire easily or lack the energy to play and participate in activities.
While several imaging techniques can be used to diagnose great vessel anomalies, MRI is often preferred, particularly in neonates. This is because MRI offers superior visualization of soft tissues and blood vessels without the use of ionizing radiation, which is a significant concern in young children.
Furthermore, MRI can provide detailed 3D images of the heart and surrounding structures, allowing for a comprehensive evaluation of the anomaly and its impact on blood flow. This detailed information is crucial for planning appropriate treatment strategies, especially in complex cases.
Example: Double Aortic Arch
- Complete double arches
- 4 vessel sign
- Descending aorta on left (opposite larger Rt arch)
Example: 40 yr old w/ dysphagia
Right Aortic Arch Anomalous Left Subclavian Artery

Example of transposition of the great arteries, where the aorta emerges from the right ventricle and pulmonary artery emerges from the left ventricle.
|
This has a typical appearance, where the aorta and pulmonary artery are parallel to each other. |
In addition, this particular example not only also has a right aortic arch, but it also shows an anomalous left subclavian artery originating from the pulmonary artery. |
There was also a patent ductus arteriosus. |
|
Finally, the pulmonary valve is bicuspid, rather than the usual tricuspid valve. |
The whole MRI exam was done without any sedation or anesthesia, and of course without ionizing radiation. It provided information not only about the anatomy, but quantified the flow in the vessels of interest. Further, it provided a quantitative assessment of the function of ventricles. |
Example: Left Atrial Appendage Aberrant Right Subclavian Artery
Kommerell diverticulum

Example: This is a right aortic arch (long arrow), an anomalous left subclavian artery with a diverticulum of Kommerell (short arrow), that together constitutes a vascular ring. Notice the tracheal (dashed arrow) is compressed in the ring.


Example: Volume rendering from a CT scan on a child with an aortic coarctation (red arrow)

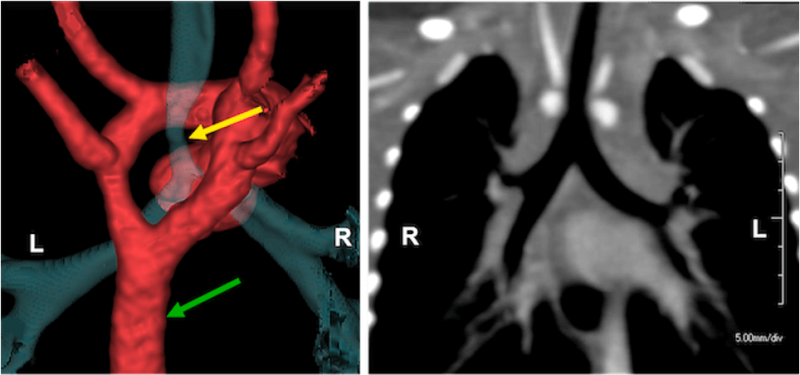
Example: Anomalous left pulmonary artery (arrow) arising from the right pulmonary instead of the main pulmonary artery (dashed arrow), which is called a pulmonary sling. The trachea (short arrow) is narrow.

